The Why and How of Radial Access
for Complex PCI
Expert Insights
Many complex cases* traditionally
approached via femoral, are now
achievable with radial access.
*Complex cases: complex bifurcation,
left main, CTO, calcified vessel
Radial access is a viable option for
cases
where the femoral route
proves difficult.
Clinical Evidence
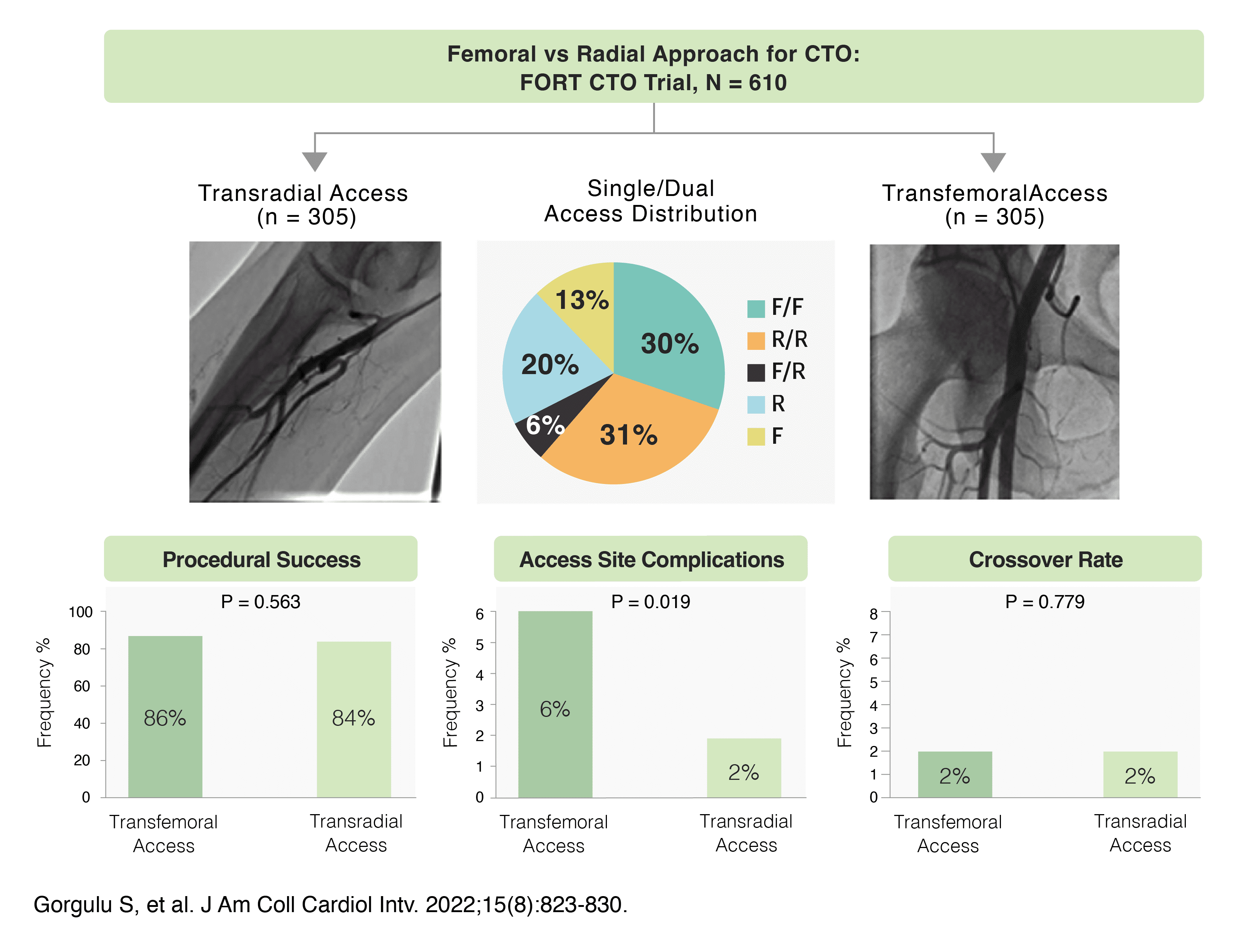
FORT CTO Trial
FORT CTO trial showed that TRA was noninferior to
TFA for CTO PCI
but had fewer access-site complications.
* J Am Coll Cardiol Intv 2022;15:823-830
Tips for Procedural
Success
Physician
Physician
- What points should I consider when attempting radial access for complex PCI?
- Start by building your skills on simpler cases before attempting complex ones. Remember,
treating PCI simply, safely and swiftly remains crucial even in complex cases.
- How do you decide when to use the transradial approach?
- The key is assessing the radial artery’s accessibility.
Typically, this is done with an Allen test or Barbeau test.

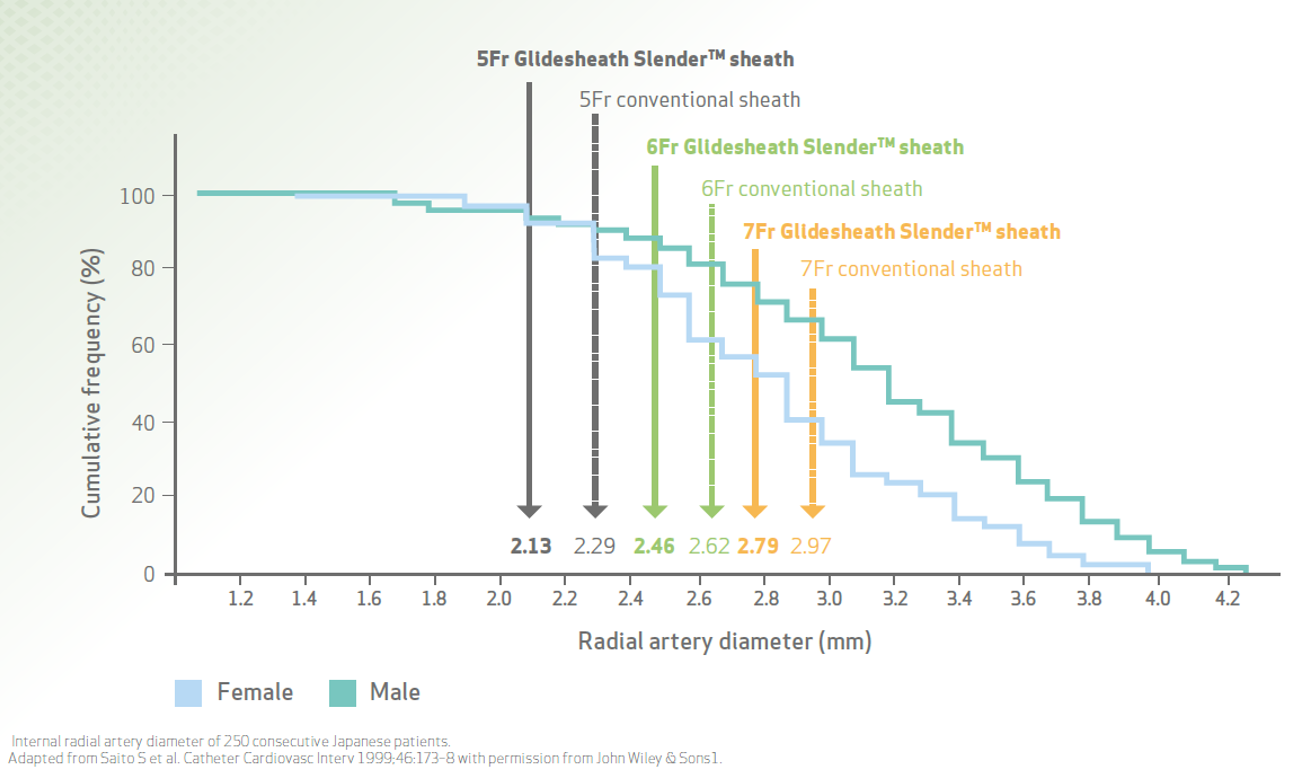
- Can you explain the relationship between the sheath size and vessel diameter?
- Sure! The graph below sheds light on the relationship between the two. You can determine vessel size using ultrasound, which, according to some data, can also improve puncture success rate.
If ultrasound is not an option, using contrast and fluoroscopy is a viable alternative.Figure 1: Thin-wall technology expands radial access for more patients.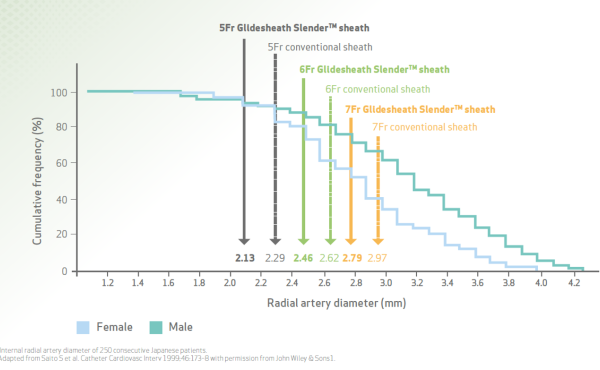 Figure 2: Ultrasound guidance improves the success and efficiency of radial artery cannulation. 1
Figure 2: Ultrasound guidance improves the success and efficiency of radial artery cannulation. 1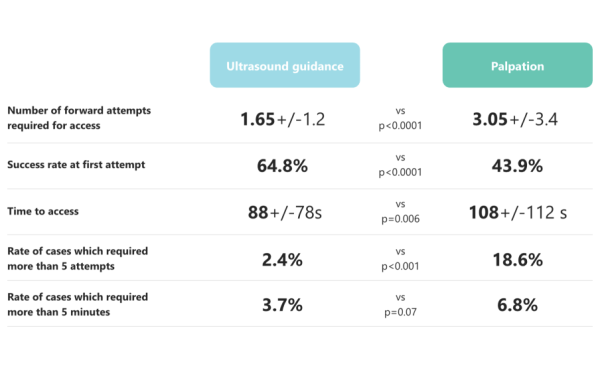

- I’m concerned about spasms during radial access for complex PCI.
How can I mitigate the risk? - Talking to the patient, helping them feel at ease, coupled with a good local anesthetic can contribute to lower spasm risk.
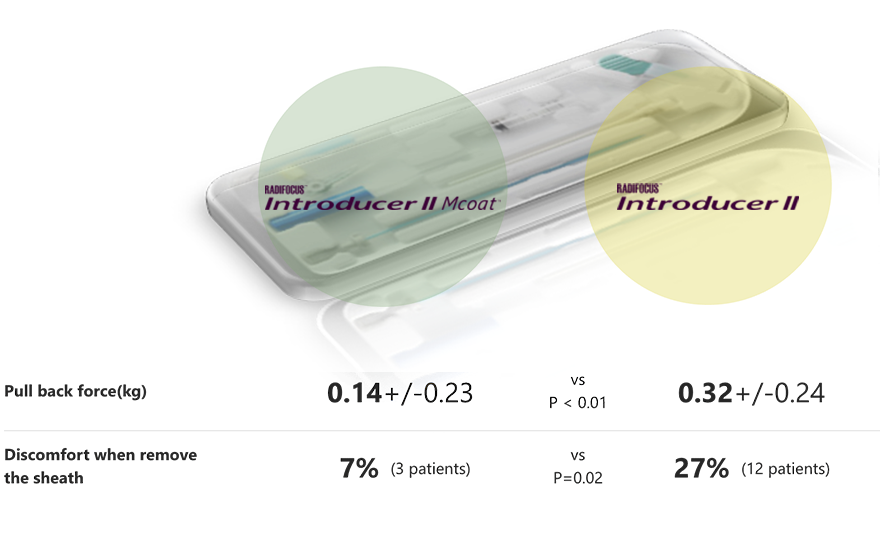
There’s also data to suggest that a hydrophilic-coated sheath can be effective too.Image 1: Avoiding excitement of the sympathetic nerves reduces somewhat the risk of
vasoconstriction.Evidence 1: Compared to uncoated sheaths, hydrophilic coated sheaths reduce the incidence of radial artery spasm.2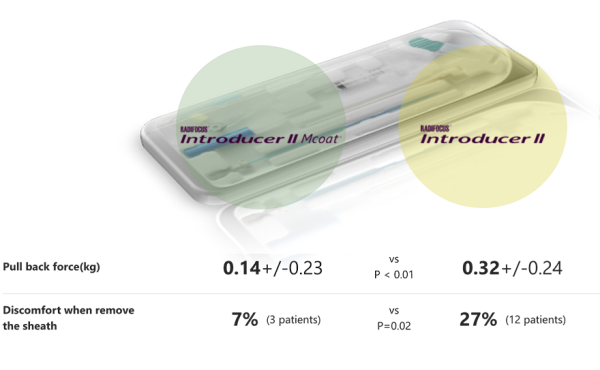
Hydrophilic coated sheath reduced the sheath removal pull back force and discomfort of patients when spams happened.3
- How can I avoid complications, like injuring the vessel or accidentally entering a branch, when inserting the guidewire and catheter?
- Using fluoroscopy can make a big difference. It lets you visually track the movement of the wire and catheter within the vessels.
Some colleagues also suggest inserting an inner catheter or multi-purpose catheter between the guide catheter and guidewire, to minimize the chances of damaging the vessel wall.Fluoroscopy image
- What about back-up support? What is an effective way to achieve it with radial access?
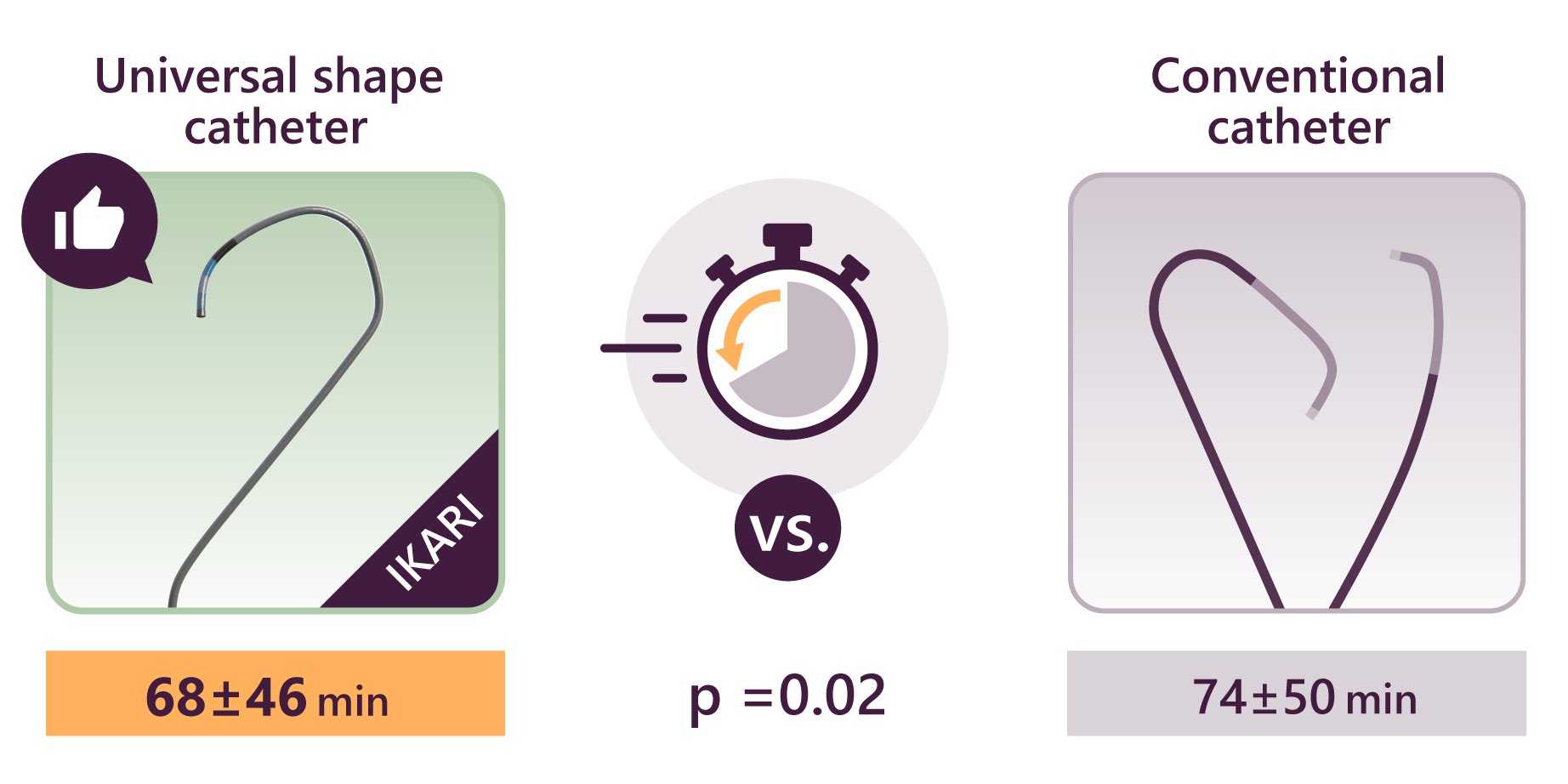
- One approach is to use a guiding catheter to establish a stable position. Using an active support catheter like Ikari left makes this easier to achieve. In fact, Ikari left not only enhances back-up support, but also contributes to reduced time in STEMI, making it a very versatile shape.
BR and BL curves are also useful for back-up support, and using a passive support guiding catheter can further enhance your back-up force.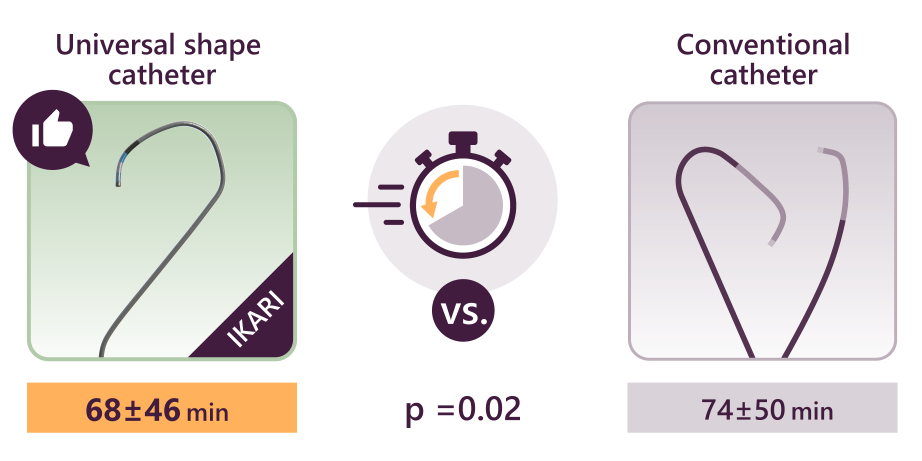
- What other methods are there for generating back-up support in radial access?
- Some alternatives include
accessing the left radial artery, using anchor balloons, support wires, or guide extensions.
All of these can be effective for creating back-up.
- Thank you, this has been very informative.
Do you have anything else you’d like to share? - I hope these tips help you feel confident to choose radial approach even in complex cases.
Supervised by Takashi Akasaka Emeritus Professor, Wakayama Medical University
Terumo IS Medical Adviser
Recommended products
-
Guiding Catheter

Heartrail™ II
Heartrail™ II will improve your back-up force when using Ikari curves right and left during transradial interventions.
-
PTCA Balloon

Ryurei™
Ryurei™ semi-compliant PTCA balloon catheter has superior crossability thanks to the combination of low distal profiles and Terumo's hydrophilic Mcoat™.
-
PTCA Guidewire

Runthrough™ NS family
Runthrough™ NS PTCA Guidewire supports a wide range of PTCA scenarios, from serving as a workhorse to tackling challenging cases.